‘The Social Impacts of Long COVID’ online symposium I convened was held on 5 March 2024. It featured presentations from Mexico, the USA, the UK, the Netherlands, Switzerland, Australia and New Zealand.
The videos of the 18 presentations in two sessions (nine presentations in Session 1, nine in Session 2) can be found on YouTube for viewing: Session 1 here and Session 2 here.
The list of presentations is below:
Session 1:
Long COVID and the (mis)uses of restitution narrative: Mark D M Davis, Monash University, Melbourne, Australia
The long haul: contested histories of Long COVID and ME/CFS in Australia: Kathy Anderson, University of Sydney, Australia
Australian experiences of socially and politically mediated determinants of health equity following COVID-19 infection: Danielle Hitch, Sara Holton, Bec Downing, Krishna Vakil, Catherine Bennett, Deakin University, Melbourne, Australia
Long COVID in The Conversation – the role of an academic journalism publication in media coverage: Lawrie Zion, Kate Stodart, La Trobe University, Melbourne, Australia
Unveiling the socio-health effects of long COVID in adult population in Northwest Mexico: Marisol Grijalva-Castro, Juana María Meléndez Torres, Research Centre in Food & Development, Hermosillo Sonora, México
The profound impact of long COVID on societal structures: governmental non-intervention and the role of social determinants of health: Pantéa Javidan, Stanford University, San Francisco, USA
The economic burden of long COVID in the United States: evidence from the panel study of income dynamics: Matt Mazewski, Rutgers University, New Jersey, USA
The debilitating discourses of long COVID: the public pedagogies of sporting bodies: Matt Ventresca, Georgia Institute of Technology/Australian National University, Canberra, Australia, Mary McDonald, Georgia Institute of Technology, Atlanta, USA
We will not be silent: patients speak out about the role of epistemic injustice in erasing evidence of Long COVID in Australia: Pippa Yeoman, University of Sydney, and member of the Australia Long COVID Community, Robin Austin, member of the Australia Long COVID Community, Su Mon Kyaw-Myint, member of the Australia Long COVID Community, Kirsty Yeates, Australian National University, Canberra, member of the Australia Long COVID Community, Ruth Newport, administrator of the Australia Long COVID Community, Australia
Session 2:
The Double-Bind: long COVID and the experience of cultural forgetting: Mary Zournazi, UNSW Sydney, Australia
A qualitative account of psychological adaptation in long COVID: Joanne Wrench, Austin Health, University of Melbourne, Jacquie Eyres, Austin Health, University of Melbourne, Kerrie Clarke, Austin Health, University of Melbourne, Centre for Mental Health Learning, Victoria, Genevieve Rayner, Centre for Mental Health Learning, Victoria, Australia
Validating long COVID with data: self-tracking experiences and practices: Sazana Jayadeva, University of Surrey, UK, Deborah Lupton, UNSW Sydney, Australia
Living with the virus: an autoethnography of the traumatic experience of long COVID: Vivienne Matthies-Boon, Radboud University, the Netherlands
Establishing a Long COVID Registry – early results and future research avenues: Paula Lorgelly, University of Auckland, Jenene Crossan, Experience & Long COVID Support Aotearoa, Andrew McCullough, University of Auckland, Aotearoa/New Zealand
“This isn’t a life”: an analysis of HRQoL in a cohort of individuals with long COVID symptoms: Paula Lorgelly, University of Auckland, Jenene Crossan, Experience & Long COVID Support Aotearoa, Andrew McCullough, University of Auckland, Aotearoa/New Zealand
Medical ambivalence and long COVID: the disconnects, entanglements, and productivities shaping ethnic minority experiences in the UK: Damien Ridge, University of Westminster, London, UK, Alex Broom, University of Sydney, Australia, Nisreen A. Alwan, University of Southampton, University Hospital Southampton NHS Foundation Trust, UK, Carolyn A. Chew-Graham, Keele University, UK, Nina Smyth, University of Westminster, London, UK, Dipesh Gopal, Queen Mary University of London, UK, Tom Kingstone, Keele University, UK, Patrycia Gaszczyk, University College London, UK, Samina Begum, University of Westminster, London, UK
Long COVID Times: An X (Twitter) informed rhythmanalysis of the complexity of pacing in chronic illness: Sam Martin, UCL/Oxford, Emma Uprichard, University of Warwick, UK
Long COVID consultations between medical clinics and modern healing rituals: a case study in Switzerland: Marjolaine Viret, Francesco Panese, University of Lausanne, Switzerland
The Social Impacts of Long COVID online symposium is taking place on 5 March, with 18 presentations spread across two sessions – one in the morning, one in the evening (Australian Eastern Standard Time). The program has been organised to best fit the time zones of presenters, who hail from Australia, New Zealand, Mexico, the USA, the UK, Switzerland and the Netherlands. Several presentations involve co-authors who have lived experience of Long COVID.
Registration is free and open to all. Details are here, including list of papers and presenters.
I have just made two submissions to the Australian government ‘COVID-19 Response Inquiry’.
The first submission summarises relevant findings from my four-year ‘Australians’ Experiences of COVID-19′ project. The submission can be downloaded below.
The second submission, written with Dr Kerryn Drysale, provides relevant findings from our project ‘Diverse Experiences and Understandings of Immunity in the Pandemic Age’. It can be downloaded below.
Convened by Professor Deborah Lupton, Vitalities Lab, Centre for Social Research in Health and Social Policy Research Centre, UNSW Sydney
This online symposium examines the social impacts of long COVID across a range of geographical locations and socioeconomic contexts.
Abstracts for possible presentations are invited from researchers on the following topics or any others related to the social impacts of long COVID:
How living with long COVID affects people’s identities, social and family relationships, life opportunities and inclusion in society
The economic impacts of long COVID
How long COVID is affecting workplaces and educational settings
How people with lived experience of long COVID are supporting and learning from each other
Long COVID activism
Media portrayals of long COVID
Arts-based and other creative responses to the experience of long COVID
To submit an abstract for consideration, please email Deborah Lupton (d.lupton@unsw.edu.au) with a description of your proposed presentation (around 200 words in length) as well as a presentation title and the name/s and affilation/s of the presenters. Deadline for abstracts: 12 midnight in your time zone, 1 February 2024.
Once I see what time zones accepted presenters are in, I will try to structure the time of the event so that it fits presenters’ (and my) time zone as well as I can.
I have just published the findings of Stage 4 of my ‘Australians’ Experiences of COVID-19′ project. The summary and key findings from this survey are provided below. The entire 25-page report is available for download here.
The national online survey findings reported in this report are from the most recent stage of the ‘Australians’ Experiences of COVID-19’ project. Conducted in mid-September 2023, this representative survey investigates 1,000 Australians’ experiences of COVID-19 and preventive practices such as vaccination and face mask wearing, their perceptions of COVID-19 risk, who they think are the most trusted sources of COVID-19 information and their views on the federal and their state/territory governments’ current management of the pandemic. The survey results show that the pandemic continues to badly affect Australians in terms of accumulated infections and prevalence of long COVID. Yet respondents were equivocal about the extent to which COVID-19 is a continuing risk to Australians. For the most part they were not strongly supportive of continued preventive actions against infection such as face mask wearing and vaccination. They did not hold high trust in any COVID-19 information source, including medical experts and scientists. Respondents were divided about how well their governments were managing the pandemic.
Key findings
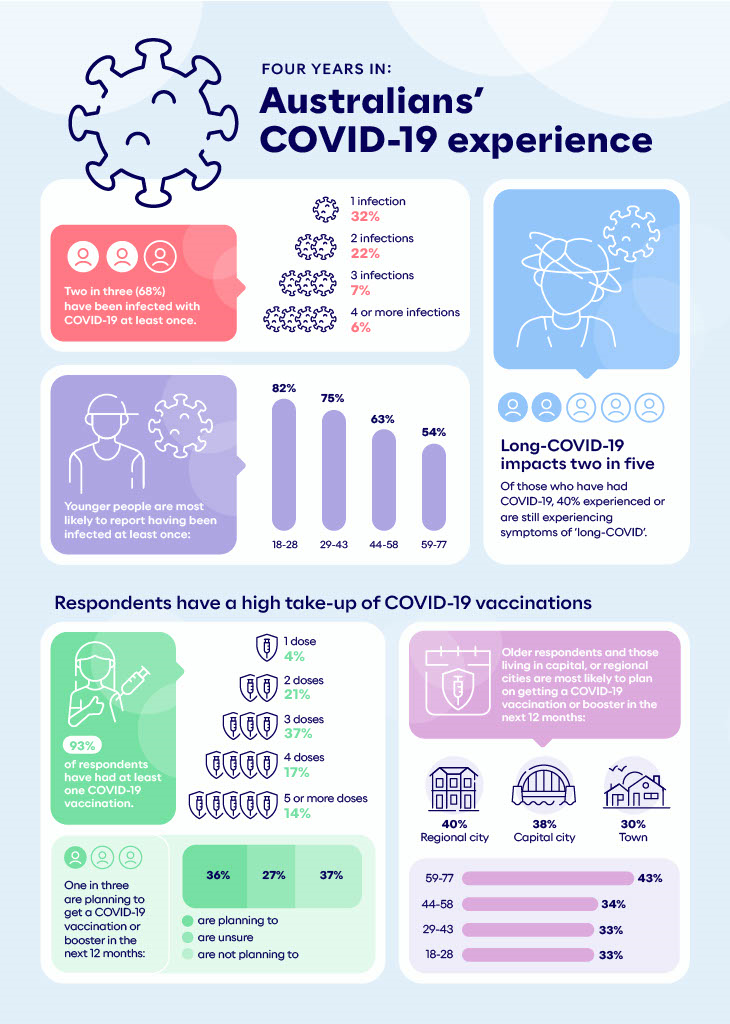
More than two-thirds of respondents (68%) reported having had at least one COVID-19 infection to their knowledge. One third (32%) reported one infection. A further 22% reported two infections, with a total of 13% experiencing three or more. Younger people reported more infections than older people, as did those in the middle household income category.
Of those who reported COVID-19 infections, 40% had experienced long COVID. More younger people experienced long COVID symptoms, while far fewer people on the lowest household income level reported long COVID.
The respondents reported a high take-up of the first three COVID-19 vaccines. The vast majority (93%) responded they had been vaccinated, with 21% having had two doses and 36% reporting three doses. However, after three doses, the proportion drops considerably.
Responses were mixed concerning plans for future COVID-19 vaccination. A total of 36% said they were planning to get another vaccine in 12 months, a similar proportion (37%) said no, and 27% were unsure. Those in the oldest age group were more likely to say that they were planning to get a further COVID-19 vaccination, as were people living in a capital city or regional city.
Face mask wearing as a personal practice was low. Only 9% of respondents said that they always wore a face mask to protect themselves against COVID-19 when inside public places. A further 26% said that they sometimes used a mask in these settings. This is a combined total of just over one-third of respondents (35%) who were still masking at least sometimes. Younger respondents were more likely to wear face masks than those in the older groups, as were those in the middle income category.
Support for face mask mandates for healthcare workers while at work was higher, with 58% in at least partial support. Here again, younger people and those in the middle income category were more supportive of mandating face masks for healthcare workers.
Doctors were considered the most trustworthy sources of COVID-19 information (60%), followed by experts in the field (53%), Australian government health agencies (52%), global health agencies (49%), scientists (45%), community health organisations (35%), Australian government leaders (31%) and other healthcare providers (28%). News reports (17%), friends and family (13%), social media (7%) and religious institutions (3%) were considered the least trustworthy. Older people were more likely to trust doctors and Australian government health agencies. The youngest group was the least trusting of scientists and experts in the field. Those in towns were less trusting of Australian government leaders, global health agencies and experts. Those in the lowest income category trusted news sources more than those in the other categories. A greater percentage of respondents in the two higher income categories said they trusted global health agencies.
A slight majority (59%) thought that COVID-19 was still posing a risk to Australians: 17% said definitely, while a further 42% saw COVID-19 as somewhat of a risk. This left 28% who did not view COVID-19 as much of a continuing risk, and 13% who thought it not a risk at all. The oldest age group saw COVID-19 as more of a continuing risk to Australians than did the younger groups, as did respondents located in regional cities and towns and those in the middle income category.
Respondents were mixed in their assessments of how well their federal and state/territory governments were currently managing COVID-19. They were evenly divided between positive assessments (36% for both federal and state/territory governments) and more equivocal assessments: 34% (federal) and 32% (state/territory). The youngest and oldest age groups were least positive about their governments’ management of COVID-19. People in towns were less positive than those in capital cities or regional cities. People with the middle levels of household income were more positive than those in other income categories.
Throughout the COVID pandemic, I have been an advocate for ensuring the events held by universities, including conferences, seminars and talks open to the general public, are safe and accessible. I have repeatedly called for events organisers and venue managers to do their best to make events COVID safe (mostly using Twitter/X to do so, but also sending emails to organisers).
As I wrote in a piece for Croakey this week, misinformation and lack of visibility about the continuing risks posed by COVID is rife across all sectors of life. As a consequence, fewer people are realising just how serious the risks are, even while new viral subvariants continue to emerge and medical research on the impacts of even ‘mild’ COVID infection (long COVID) is continually being published (see, for example, a recent editorial in the British Medical Journal ).
In addition to providing education on long COVID to the biomedical community, we need a public communications campaign that informs the public about the risks and outcomes of long COVID.
In the absence of government-run campaigns, have been doing my best to engage in public communication about COVID risk – including to my academic colleagues. Three months ago, I published a set of guidelines on this blog to help organisers ensure that their events would not become super-spreader occasions. These guidelines offer opportunities for event organisers to expand access and improve inclusion not only for people who want to avoid COVID infection but also those who are disabled, are carers, have little travel funding or live in countries where visas for travel to conferences are denied, or who want to reduce their carbon footprint.
Advocating for COVID safe and otherwise more accessible academic events is proving an ever more serious challenge in an information environment (even at universities) in which it seems to assumed that the worst of the pandemic is over and many protections for event attendees have either been dropped or are not adhered to. For example, ‘strong recommendations’ for people to wear masks to protect themselves and each other seem to be little observed.
Over the past year, I had seen many reports of academic events offering no online options for participation. I had heard of many conferences where people had tested COVID positive while attending or soon after returning home. But what is happening at the writers’ conference being held at Middlebury College’s Bread Loaf campus in Vermont, USA, really alarms me. Reports have come through on Twitter/X about over 10% of attendees reporting COVID infections. Those infected are reporting that they have been given little support by the event organisers, have been sent home while ill and infected, and that the rest of the conference was continuing with few mitigations in place to protect those still on site.
I made it home frm “the mountain” somehow propelling myself home on a 6hr drive in a fugue state. I am so very, very sick. So much water and advil and rest and still, can hardly drag myself out of bed to pee. If I get long covid I’m going to be SO pissed. https://t.co/wIiQCnc5CI
Bread Loaf has sent its covid+ workshoppers home w/o regard to increasing viral transmission unlike @LambdaLiterary, @sewaneewriters & @Tin_House, each of which had robust covid protocols. it’s clear which conferences prioritize community safety & which are just a cash grab. https://t.co/Dnj9CxGJt2
Is this the future of academic conferences? Little care taken to protect attendees, covering over the harsh realities of what has happened to those who were infected, expecting people to leave immediately, even when they are very ill and pose a risk to anyone they may come into contact while travelling home?
It seems it is time to redouble my efforts to draw attention to these issues. We need to #MakeConferencesCOVIDSafe. The lives and health of academics and other knowledge workers (such as these talented writers) – across the age span and seniority levels – should not be placed in further jeopardy.
The third revised edition of my book Risk, first published in 1999, and second edition published in 2013, is now out. The book has been extensively revised and expanded to take account of the risks that have emerged over the past decade.
A link to the book on Routledge’s website is here and the Google Books preview is here.
Below is the Preface I wrote for the third edition.
In the 1990s and into the early years of the twenty-first century, risk was a key word in both public forums and academic research. The word ‘risk’ was used across social domains and institutions. The sociocultural and political aspects of risk and identifying the reasons for this intensification on risk identification, communication and management were a major preoccupation in the social sciences. The release in 1992 of the English translation of the German sociologist Ulrich Beck’s book Risk Society: Towards a New Modernity was one of the initial impetuses for this academic focus. Simultaneously, however, the scholarship of French philosopher and historian Michel Foucault on the care of the self and the governance of populations, and that of British social anthropologist Mary Douglas on the symbolic dimensions of risk cultures began to be taken up by social researchers and theorists. Their writings were extensively used by others exploring the reasons for why risk had become such a vibrant concept and discussing the implications for social identities, group membership and the management and control of diverse societies.
I wrote the first edition of Risk, published in 1999, for Routledge’s Key Ideas series. In the book, I laid out a schema in which I categorised the Beck approach as ‘the risk society’ perspective, Foucauldian insights as ‘the governmentality’ perspective and Douglas’ scholarship as ‘the cultural/symbolic’ approach. I elaborated on each of these three perspectives and provided examples of how they had been applied to empirical investigations into risk-related understandings and practices. The second revised edition of Risk came out in 2013. In updating the book, I added discussion of some additional theoretical perspectives, discussed some topics that had newly been labelled as risks and included findings from empirical studies that had been conducted since the first edition was published.
It is now a quarter of a century since the first edition of Risk appeared. Over this time, I have noticed that the topic of risk has gradually taken a back seat in social and cultural theory and research, despite its continuing salience to major problems and crises across the world. There have been various ‘turns’ emerging in theory over this time that in some ways have supplanted the ‘risk turn’. The ‘affect turn’ and the ‘materialism turn’ are two key developments. Some scholars have attempted to bring these bodies of theory together by examining the affective or sociomaterial dimensions of risk. However, thus far, this scholarship has largely remained on the fringes of risk research.
In revising Risk for its third edition, I therefore thought it important to make a strong call for a ‘re-turn’ to sociocultural risk theory in a way that incorporates insights from these theoretical developments and addresses the latest catastrophes besetting the world. At the time of writing, the world is faced with frightening disasters and emergencies. The Russian invasion of Ukraine that commenced in early 2022 continues unabated, with no clear end in sight, while the crisis affecting displaced people in other nations such as Syria, Venezuela, South Sudan and Afghanistan continues to create hardship, poor health and uncertainty for these groups. The COVID-19 crisis, confirmed as a pandemic by the World Health Organization in March 2020, is still raging globally. Citizens of the world’s most populous country, China, are facing rapid spread of the disease for the first time, following its leaders’ decision to drop many of the strong prevention strategies that have successfully controlled the outbreak in that nation. The climate emergency and associated risks of environmental degradation, loss of biodiversity, emerging diseases affecting humans and other animals, and devastating natural disasters such as wildfires, floods, droughts and landslides has yet to be properly addressed by governments, national leaders and peak global organisations. There are global food and fuel shortages triggered by the war in Ukraine, other disruptions in supply chains due to the COVID emergency, and many nations face an economic recession and severe cost of living crises.
Together, these emergencies appear so intractable and unsettling as to be labelled as constituting a ‘permacrisis’: a term chosen as Collins Dictionary’s word of the year for 2022. Yet we are living in a world in which the existence of risk is constantly debated, misinformation and disinformation are rife and spread quickly and easily through online media, and where governments and institutions continue to avoid taking decisive action even when there is general agreement that a serious threat exists. Understanding how people, social groups and social organizations understand, respond to and act on threats, hazards and dangers is more important than ever. This third edition has been updated to confront these issues, including the addition of an entirely new chapter that focuses on risk misinformation, scepticism and denial, using the climate and COVID-19 crises as case studies.
We are in our fourth year of the COVID-19 pandemic, and at the same time as governments and health agencies are wanting to promote the idea that the emergency phase is over and we should all learn to ‘live with COVID’, many people are still getting infected or reinfected. Faculty and students are attending academic conferences and coming back with new COVID. This has the potential to severely affect their health into the future, as well as posing a risk to the people back home with whom they come into contact.
Conference organisers need to ensure better COVID safe conditions to protect attendees’ health. Here are some guidelines for what should be done.
Offer online options to participate in the conference. Not only will this prevent the spread of COVID through reducing exposure due to travel and conference mingling, it also provides better accessibility for people who are ill or disabled, have caring responsibilities, do not have ready access to conference funding or live in countries where it is difficult to obtain visas to travel abroad. Online options also mitigate against the significant carbon emissions and pollution caused by air travel.
Ask all attendees not to attend the conference under any circumstances if they, or any of their household members, have any infectious illness symptoms of any kind. Ensure that they know that any fees charged for the conference are fully refundable in these circumstances so that people are not tempted to participate because they feel they will have wasted money.
Have rapid COVID tests available free at the venue, and encourage participants to regularly test themselves while at the conference and in the days after the conference.
Only use venues where there are effective systems in place to ensure clean indoor air. Undertake a risk assessment for airborne infection before you book and confirm the venue. Check the quality and effectiveness of all mechanical ventilation systems (HVAC) at the venue for the rate of fresh air delivery and exchange. Determine whether air purifiers or other air cleaning technologies are in place or can be hired for the event. Check if there are windows in the conference rooms that can be opened to allow for fresh air to enter. Consider making sure all doors to the venue and internal rooms can be left open to allow fresh air to enter. Use an air quality monitor (Aranet4 or similar) to check the air quality in the venue spaces periodically throughout the conference, and take steps to improve it if there is a problem. In short, do everything you can to ensure that the venue has clean air systems in place to reduce the risk of airborne viral transmission. See here for CDC’s guidelines on ventilation in buildings.
Preferably, the wearing of respirator masks (N95 or better) should be mandated for all attendees. This will deal with the peer pressure that often stops people from donning a respirator (“I don’t want to look different”, “No-one else is wearing a mask, why should I?”). If this is not possible, respirator mask wearing should be strongly recommended, and free N95s should be made available at the venue for every attendee. Conference organisers should model wearing N95s at all times.
All refreshments should be made available in an outside space only.
Further resources and information here from The COVID-19 Safety Pledge (UK) website
This time three years ago, all Australians were experiencing the one and only national lockdown that was implemented in our nation to contain the COVID-19 pandemic (further lockdowns were localised, and for some Australians, this national lockdown was the only extended one they experienced over these years). Restrictions began to be introduced by the Commonwealth and state governments in mid-March 2020 and as COVID cases began to drop and community transmission became well controlled, these measures were gradually eased from mid-May 2020.
The national lockdown was a stressful, frightening and difficult time for many people, particularly those who lost their jobs, were dealing with educating their children at home or struggled with feelings of social isolation. However, some Australians found some silver linings or discovered that their lives were hardly changed by the restrictions. This was a time where everyone was taking the risks posed by COVID-19 very seriously, and Australians for the most part did their best to engage in the recommended measures to ‘stop the spread’. (See here for my publications reporting on Australians’ experiences, based on interviews with people across the nation.)
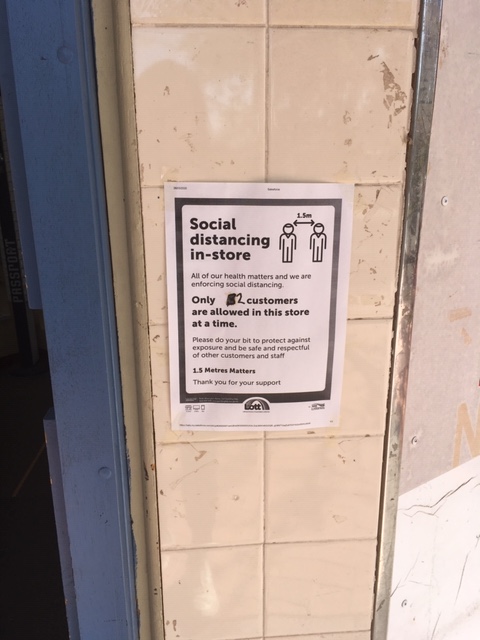
The markers of experiences of this first lockdown were mostly ephemeral: supermarket shelves stripped of toilet paper, hand sanitiser, pasta, flour and other goods, signs warning people to distance from each other, and to wash their hands, cover coughs and sneezes, and informing potential customers that businesses were closed, or newspaper ads and pamphlets distributed to householders by governments and businesses.
As a social researcher of health topics, I began taking photographs of my surroundings, to keep a record of life during COVID. I have published an essay using some of these images (but it is behind a journal paywall). Below, I include several of these photos (all captured with my smartphone in April 2020) as a reminder for everyone of this pandemic past, as we move into an era in which forgetting the continuing risks posed by COVID-19 seems to be a major cultural and political phemomenon.
As we can see from these images, words such as ‘protect’, ‘together’, ‘help’, ‘respect’, save lives’, ‘community’ and ‘stay safe’ were commonly used to highlight the importance of following these rules and acknowledge that ‘we are all in this together’. Whereas once the dominant message was to ‘protect yourself and others’, now it is ‘if you feel unsafe or anxious, stay home or wear a mask’. The sense of community and feelings of care have largely fractured into a ‘you do you mentality’ – or worse, into bitter hostility against people who continue to take preventive measures to protect themselves and others, such as mask wearing.
The third in my series of books about the social aspects of COVID-19 is out today. COVID Societies: Theorising the Coronavirus Crisis can be ordered from Routledge here and a preview of its contents can be viewed at Google Books here. The abstracts for each chapter are listed below.
INTRODUCTION: COVID societies
The COVID-19 crisis has provoked intense and far-reaching socioeconomic changes globally as well as posing a major threat to human health and wellbeing. This introductory chapter introduces the rationale for the book, addressing the question of why sociocultural theories and historical perspectives are so important to make sense of how the COVID catastrophe erupted and created so much turmoil worldwide. The chapter also provides an outline of the content of the remainder of the book, detailing the topics and theoretical perspectives on which each of the ensuing chapters focus. These include discussions of the political economy perspective; biopolitics; risk society and cultures; gender and queer theory; and more-than-human theory.
1 COVID IN CONTEXT: Histories and narratives of health, risk and contagion
Major new or recurring infectious disease outbreaks are always accompanied by significant sociocultural and political disruptions and transformations. These crises often call into question ways of viewing and living in the world, as well as exposing and entrenching forms of social discrimination and inequalities. This chapter provides an overview of the historical, sociocultural and political contexts of the COVID-19 crisis. Medical historians, sociologists, anthropologists and cultural geographers have shown that social, cultural and political responses to the emergence or return of deadly pathogens often bring to the surface hidden, unacknowledged or long-established beliefs and practices. The chapter demonstrates how these perspectives have offered much of value in relation to the analysis of the sociocultural and political dimensions of previous serious infectious diseases. This discussion is followed by an account of how the new virus SARS-CoV-2 and the new disease COVID-19 emerged in the early months of 2020 and developments in the pandemic throughout 2020 and into 2021.
2 THE MACROPOLITICS OF COVID: A political economy perspective
Political economy critiques adopt a macropolitical perspective, drawing on Marxist theory as well as feminist critiques, critical disability studies, critical race theory and postcolonial theory to highlight the social determinants of health and healthcare and the role played by medical expertise and authority in society. A political economy perspective incorporates the discussion of social justice issues, inequalities and the exacerbation of socioeconomic disadvantage caused by the pandemic, including the disproportionate effects on low-income countries and marginalised social groups. Indeed, some commentators have argued that the COVID-19 pandemic has surfaced a ‘crisis of care’, in which the failings of neoliberal political and privatised approaches to public health surveillance systems and healthcare delivery across the world have been shockingly revealed. This chapter shows how neoliberal and free market capitalist political systems have been called to account and disrupted by the COVID crisis but have also operated to protect the privileged and further entrench inequalities in COVID societies. The concepts of medical dominance, the social determinants of health and globalisation are explained and applied to the COVID crisis.
3 THE BIOPOLITICS OF COVID: Foucauldian approaches
COVID-19 governance at the level of the state raises questions about how power is exerted and experienced and how it may be productive as well as repressive. This chapter delves more deeply into the complexities of these tensions and conflicts, using perspectives drawn from the scholarship of the French historian and philosopher Michel Foucault to trace the historical underpinnings of contemporary approaches and responses to the COVID crisis. Various levels of control over citizens’ bodies and movements have been exerted and rationales for limiting individual freedoms put forward to protect the health of the body politic. Foucauldian theory offers concepts for understanding these relations of power. The scholarship of philosophers Giorgio Agamben and his concepts of bare life and states of exception, Roberto Esposito and his notions of affirmative biopolitics and immunitary mechanisms, and Achille Mbembe and his writings on necropolitics is also outlined. This discussion is followed by an account of Foucauldian viewpoints on the biopolitical dimensions of COVID societies have been developed, including discussion of how these theorists analysed social and governmental responses to the crisis.
4 RISK AND COVID: Risk society and risk cultures
The COVID-19 crisis is suffused with discourses, practices and emotions related to people’s reactions to risk and uncertainty. This chapter focuses on sociologist Ulrich Beck’s risk society perspective and anthropologist Mary Douglas’ cultural/symbolic approach to risk. Concepts from Beck’s scholarship, including reflexive modernisation, individualisation and cosmopolitanism, and Douglas’ work on the cultures of risk, blame and symbolic boundary control are explained and applied in an analysis of risk and uncertainty in COVID societies. The chapter shows that the risk discourses and practices circulating within and between regions and countries globally involve an affectively compelling combination of concepts of embodiment, contagion, danger and morality. The COVID crisis can be considered both a pre-industrial, fateful event and a late modern risk society phenomenon.
5 QUEERING COVID: Insights from gender and queer theory
This chapter introduces insights from scholarship in gender and queer theory and shows how they can be productively applied to an analysis of embodiment and socialities in COVID-19 times. While contemporary queer theory has its roots in critical studies of gender and sexuality, it has since expanded well beyond these origins. There are many intersections and overlaps between gender and queer theory, and both reach into many related fields: including queer necropolitics, queer death studies, crip studies, fat studies and critical animal studies. The major precepts of these intertwined bodies of literature are explained, with reference to the influential scholarship of philosophers such as Mel Chen, Michel Foucault, Judith Butler, Elizabeth Grosz, Gilles Deleuze, Félix Guattari and Julia Kristeva. These extensions of gender and queer theory and what they offer for analysis of the COVID crisis are considered in this chapter. They critically analyse aspects of discourse, affect and embodiment to ‘queer the pandemic’: that is, to highlight disjunctures and invisibilities in the ways with which COVID has been portrayed and dealt and to provide further insights into the nature of lived experience in COVID societies. In identifying how these responses might be subject to contestation and change, contributors to gender and queer theory scholarship imagine better and more inclusive futures.
Given the intertwined dimensions of human and nonhuman relations and connections, the crushing impact of the COVID-19 crisis extends well beyond human lives and agencies. Scholars and researchers are beginning to engage with the body of scholarship that I refer to as ‘more-than-human theory’ (alternative terms used are ‘new materialisms’ or ‘the critical posthumanities’). There are various varieties of more-than-human theory. In the discussion presented here, I focus specifically on the scholarship that builds on non-western cosmologies (particularly Indigenous and First Nations philosophies) and the feminist materialism perspectives offered by western philosophers Rosi Braidotti, Donna Haraway, Karen Barad and Jane Bennett. These philosophies advance a non-anthropocentric approach to understanding human existence. The implications of this approach for understanding the complexities and dynamism of COVID societies are outlined in this chapter. More-than-human theory is applied to better understand the affective forces and relational connections that are generated with and through humans’ encounters with nonhuman agents. I discuss the assemblages of humans and nonhumans that have come together and come apart as the COVID crisis unfolded. As I show, such an approach expands the One Health perspective in productive ways.
CONCLUSION: Reflections on COVID futures
This brief conclusion chapter summarises the key insights offered by COVID Societies, and then moves towards a future-oriented discussion. It is noted that throughout the book, a series of intertwined threads cross back and forth between the macropolitical and micropolitical dimensions of COVID-19: contagion, death, risk, uncertainty, fear, social inequalities, stigma, blame and power relations. Overarching these threads are five complementary themes: the historicity of COVID societies; the tension between local specificities and globalising forces; the control and management of human bodies; the boundary between Self and Other; and the continuously changing sociomaterial environments in which the world is living with and through the shocks of the COVID crisis. At this point in the pandemic, only uncertainty seems certain. As we learn to live with and through COVID, we must work towards better conditions for people across geographical regions. Acknowledging our vulnerability and using this knowledge to better care for the more-than-human worlds in which we are emplaced is a way forward to care more deeply about ourselves and our fellow species.